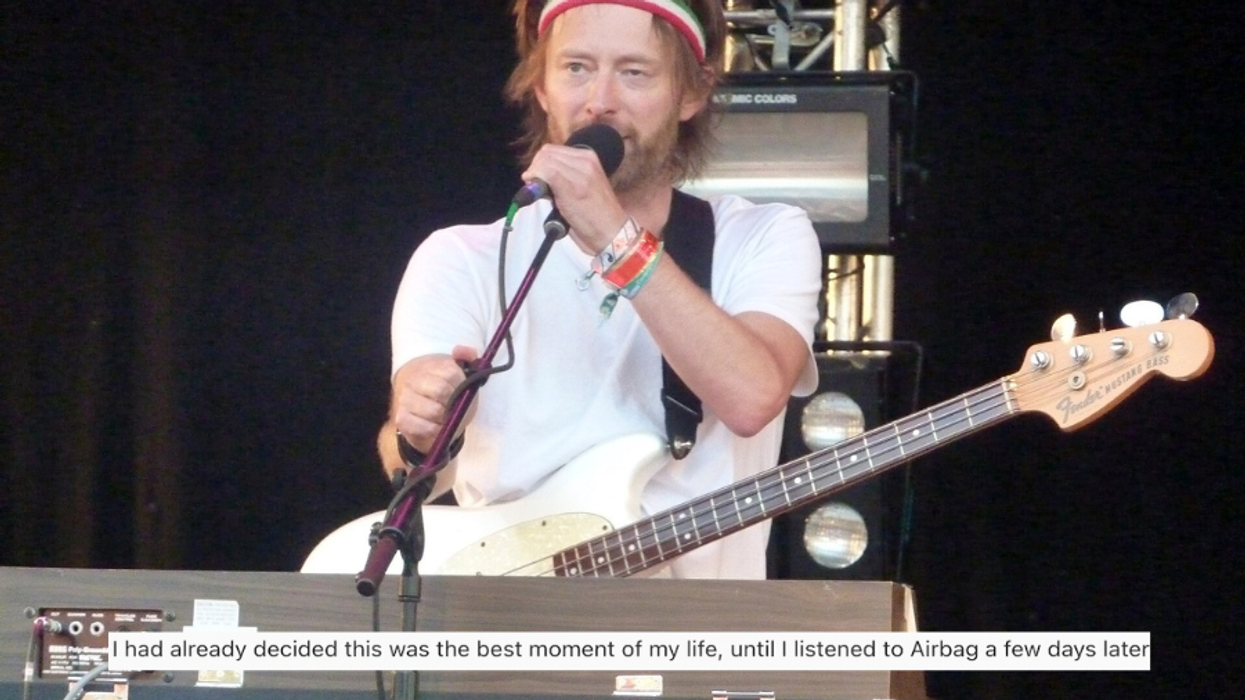


We might be on our way out of Iraq but things are just starting to pick up in Afghanistan. With record-high number of veteran suicides and rising rates of post-traumatic stress disorder and clinical depression in every branch of the armed forces, is the nation headed for a mental-healthcare crisis?On the eve of her discharge from the U.S. Navy, Annette Yover stood beneath a black sky watching fireworks explode in blooms of green and purple, yellow and red. It was July 4th, 2005, and the Navy was holding its annual Independence Day celebration at Carney Park, an American military recreation center in Naples, Italy. Yover had been stationed there for the last 18 months. A mortician at the nearby U.S. Naval Hospital, she was looking forward to a night of celebration with her friend. They spread out a blanket among crowds of other soldiers, and sat down to enjoy the show.But Yover soon noticed something was wrong. As columns of fireworks spiraled into the air, each explosion more amplified than the last, her heart rate quickened and the blood drained from her face. The repetitive booms reminded her of the mortar fire she heard while forward-deployed in Kuwait, collecting human remains from the battlefront in Iraq. The smell of sulfur triggered memories of long hours spent in the Naval mortuary, mending wounds on the bodies of dead soldiers. Her chest muscles tightened, and tears welled up in her eyes. At first her crying was subdued, escaping from her mouth in short bursts. But it quickly gave way to heaving sobs, the type that take hold of the body and forcefully wring it out."I noticed other people looking at me," Yover says now. "But I was the only one reacting. It was overwhelming, that sense of panic, that feeling of, ‘I need to get out of here.'"
Annette Yover |
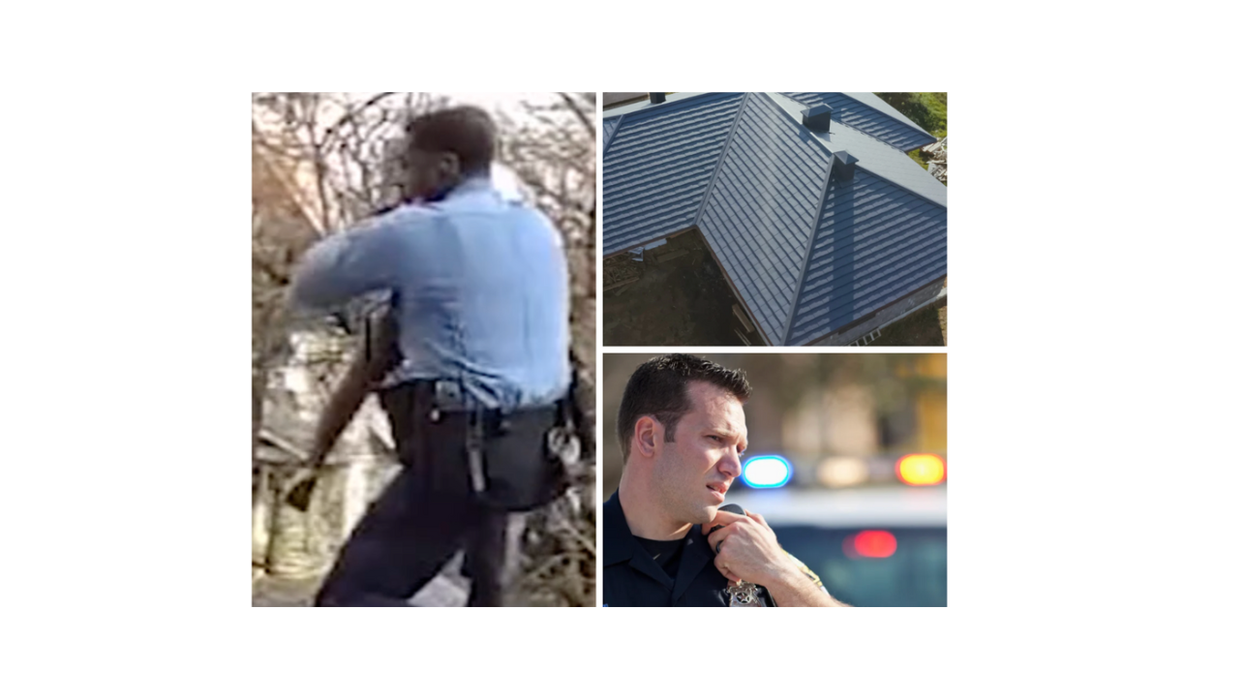
Todd Bowers |
This is the first time since the Vietnam War that the rate of suicide in the Army has surpassed the civilian suicide rate.The Army conducts mental health screenings for soldiers, but the effectiveness of that practice has come into question. Before suicide rates and the number of reported cases of PTSD began to rise, the Army gathered behavioral health data by dispatching Mental Health Advisory Teams to Iraq and Afghanistan in 2003. The MHAT assessments led to several changes in troop preparedness, most notably, the implementation of something called Battlemind training. As the Army defines it, Battlemind is designed to "help prepare soldiers and their families for the stresses of war" both pre- and post-deployment.The long-term effectiveness of Battlemind remains to be seen. Since the program's inception in 2006, a record number of suicides have been reported, as well as a growing caseload of active duty troops and veterans with PTSD and clinical depression."[Battlemind] is a good first step," says Bowers. "But it's basically trying to reduce the mental health stigma by using videos and a website." Bowers believes this is the wrong approach-that what soldiers need is dialogue between service members and with leaders. "If someone who is higher up says ‘I came back and I had some issues and I got them dealt with,' they really respond to that."In late January, the Army announced that the suicide rate of its troops had increased for the fourth consecutive year. At least 128 soldiers committed suicide in 2008-the highest count since record keeping began in 1980-with another 15 deaths still under investigation.January of this year saw 24 suspected suicides, an unusually high number-there were just five suicides in January of last year. This is the first time since the Vietnam War that the rate of suicide in the Army, about 20 deaths per 100,000 soldiers, has surpassed the civilian suicide rate.
An Army poster aimed at suicide prevention. |
"It's quite possible that the suicides and psychiatric mortality of this war could trump the combat deaths." -Thomas Insel, director of the National Institute of Mental HealthIndeed, PTSD can manifest weeks, months, or even years after exposure to a traumatic event or series of events. Common symptoms include flashbacks, recurring nightmares, hypervigilance, and panic attacks, among others. To complicate matters, the disorder often occurs in conjunction with depression and substance abuse.Further, according to Tuma, there is concern that the health care sector at large needs to be educated about the unique challenges facing this generation of veterans, as well. Veterans who seek care outside the VA system have had a very different experience than the average patients a community doctor treats, he says."Health and Human Services is trying to figure this out for the civilian sector, how many people should they expect to be knocking on the doors of community mental health centers with PTSD or depression," says Lisa Jaycox, senior behavioral scientist at the Rand Corporation and co-author of last year's study, The Invisible Wounds of War. "[They] are also really trying to think through ‘What are we going to need to be ready for?' and ‘How can we improve the system of care?'"Meanwhile, last October, the Army and the NIMH signed an agreement to conduct a five-year research study in hopes of finding intervention and mitigation strategies to help decrease suicides.What remains to be seen is how this attention from government agencies and private institutions will translate to an actual improvement in veteran care. Critics contend these efforts are coming too late. The Department of Defense's choices-such as extending tours of duty from 12 to 18 months, shortening downtime between deployments, and involuntarily extending soldiers' enlistment under the stop-loss program-are the very factors that helped create an environment ripe for an epidemic of PTSD and depression."We are going to see a massive influx of people coming home with mental health problems as a whole and really having a tough time readjusting," says Bowers. "If we can catch these people now, before they become homeless, before they rely on permanent treatment, we're going to save a lot of money and, more importantly, save a lot of lives. Veterans issues affect every single American because veterans rely on the American public for their care when they come home. They're willing to defend this nation on the battlefield but then our nation has to defend us on the home turf-that's really what I hope people pick up on."For many veterans, returning home is often a difficult, sobering experience. "After I left active service and attempted to return to civilian life, that was probably my first indication of feeling like I didn't fit in," Yover says. "I tried working at a civilian funeral home, as I had before I went into the military, and was finding it increasingly more difficult to handle the job."Though returning to the life she left behind in Arizona proved harder than expected, it was her inability to work as a mortician that upset Yover the most. "Not only did [my PTSD] change me and the way I saw things, but all of a sudden it took away my livelihood," she says. "When it impacts various aspects of your life, it feels like you've been robbed of something."Yover enlisted in the Navy following the September 11th terrorist attacks, at age 30. In the four months between enlistment and boot camp, Yover sold her home in Phoenix; left her cat in the care of a friend; and resigned from her job as a mortician at Greenwood Memory Lawn."For me, it was a very personal journey," she says. Today, Yover is an officer at the Arizona Department of Veterans' Services, where she helps veterans receive their VA benefits by shepherding them through the program. But with her military service now over, and her life dramatically altered as a result, Yover still struggles to find a sense of normality in her daily life."I think that's where the difficulty is, in retraining yourself," she says. "Someone told me that PTSD is nothing more than a memory with the volume turned up too loud. And that's essentially what it is-a bad memory."Photos of Annette Yover courtesy of Annette Yover. Photos of Todd Bowers courtesy of IAVA. Poster courtesy of the U.S. Military. Iraq photo courtesy of flickr user Army.mil.